
The Inscrutable Belief System of Involuntary Commitment
Politicians keep boosting funding to expand force in a vacuum of evidence

Two recent reports on state involuntary commitment systems, in Virginia and North Carolina, involved completely different investigative approaches. Yet both show that many people simply want to believe in the virtues of involuntary commitment—even as they struggle to grapple with the overwhelming lack of facts that might support such faith.
Meanwhile, for some of us, the available facts are enough to make it seem like the only truly sensible approach is to abolish involuntary commitment—unless and until it can be demonstrated that it actually helps more than it harms.
A Plummeting Sense of Dignity in Virginia
“Between Custody and Care: The Flawed Involuntary Commitment System in Virginia” was produced by the disAbility Law Center of Virginia (dLCV), and involved interviews and surveys of 79 people who’d recently been committed in that state.
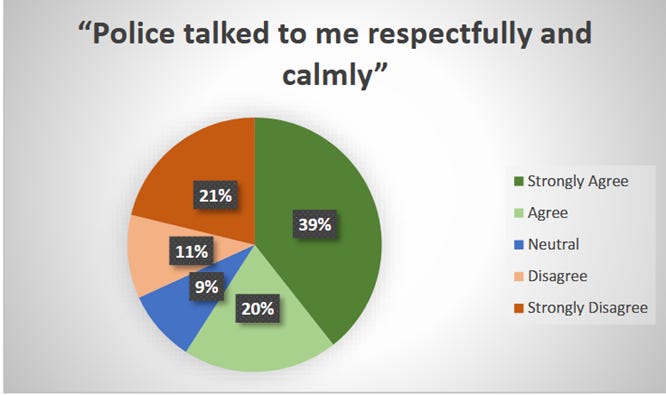
One aspect of the survey particularly caught my attention. Look at the number of people who reported that police officers treated them with respect: 59%.
A lower percentage, 52%, felt the hospital staff treated them respectfully.

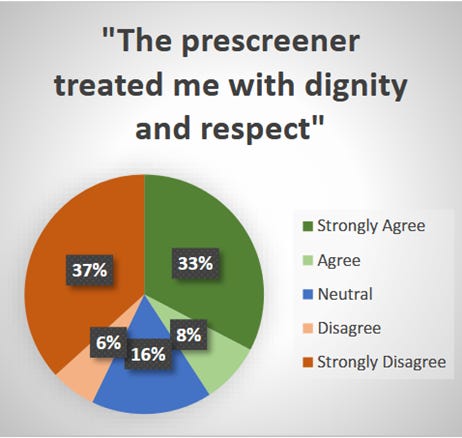
And a still lower percentage (only 41%) of people felt that the pre-screener—the person actually evaluating them for possible detention—was respectful.
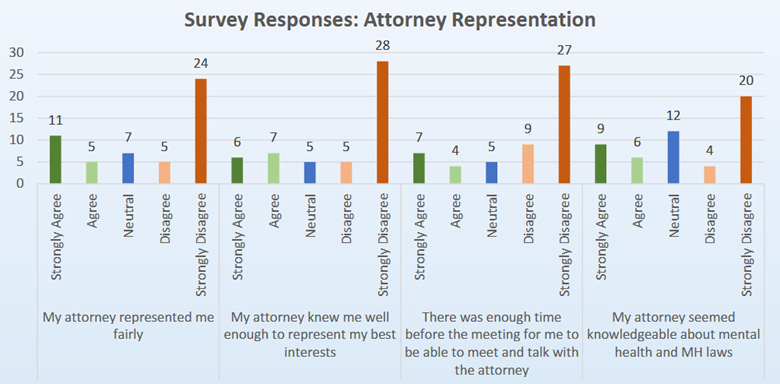
Finally, by the time they got to the hearing process, for most patients the feelings of disrespect and dissatisfaction were rocketing upwards, to the point where they were feeling shafted even by their own attorneys. Consistently less than 16% felt their attorney took enough time to get to know them or their case, or to represent their views fairly.
And even these grim numbers appear to be inflated across the board—likely by the fact that the survey respondents were somewhat forgiving to the individuals involved, even as they felt abused by the involuntary commitment system as a whole.
I suggest this because, in responses to the other survey questions, people reported a litany of problems and abuses throughout the entire commitment process.
Restraints creating disorder
Most people remained handcuffed for hours, sometimes even for days, while in police custody. “[Restraints were not rare exceptions but routine practice,” dLCV found, and “respondents shared heartbreaking accounts of traumatic and prolonged restraints, even when they did not pose any active danger.” These overuses of restraints led people to feel “panicked, pained, and as if they had done something wrong” and “increased their anxiety levels and led to injury.”
People with physical or developmental disabilities or communication impairments weren’t accommodated. Most people were never properly informed of their rights. Sixty-five percent said their attorneys did not even give them any contact information. Nearly a quarter never got an attorney at all.
Many reported that they were not able or not allowed to attend their own commitment hearings, and some said they didn’t even get hearings. Some were so heavily medicated against their will that they could not stay awake for their own hearings or, as one recounted, managed to stay awake but “were so sedated, they didn’t remember anything.”
And the appeals process was a complete sham, dLCV found: “Nearly every individual who reported that they wanted to appeal or who requested an appeal, did not hear back or was told that they could not appeal due to timeline issues.”
“I had no idea about appeals until reading this survey,” said one respondent.
In conclusion, dLCV wrote:
“Law enforcement and emergency departments are subjecting people with disabilities to prolonged, abusive and often unnecessary restraint.”
“Personnel at all steps of this process do not have the competencies needed to serve people with disabilities. As a result, they routinely violate individual rights.”
“These findings show a systemic failure of due process rights.”
What’s more, the prospects for improvement in these systems look dicey at best—one reason dLCV took this survey-based approach was because no mental health providers or government agencies are bothering to collect information on who is being affected, and how they’re being affected, by Virginia’s involuntary commitment system. “[N]o state agency collects data or assesses the process to determine whether there are patterns of concern that can be addressed,” wrote dLCV. “Without good data, the institutions involved in this process cannot possibly self-evaluate and the Commonwealth at large simply does not know what is happening to people whose civil liberties are being suspended.”
Nevertheless, at the end of all of this, dLCV made the following recommendations:
—policy changes to limit the use of restraint;
—enhanced training for all personnel involved in the process; and
—protocols and plain-language materials to ensure that people are adequately informed of the process, as well as their rights.
But is there really anything here that inspires much confidence that such recommendations, even if legislatively passed, would be properly implemented? The corruption and abuse is so deep, systemic, and routine, it seems to demand calling for an immediate halt to all involuntary commitments—unless and until all of these problems are rectified and it can be demonstrated that involuntary commitment is actually helping people.
This tension between people’s clear observations of how severely corrupt and damaging the involuntary commitment system is at its core, and a faith many of them nevertheless still place in it, is even more striking in the latest report from North Carolina.
Revolving Doors Into Chaos and Calamity in North Carolina
The General Assembly of North Carolina’s House Select Committee on Involuntary Commitment and Public Safety took an entirely different investigative approach from dCLV’s in Virginia.
The Committee met five times during 2025, and invited presentations from a slew of people studying and/or working in the state’s involuntary commitment system, including psychiatrists, law enforcement officers, magistrates, academic researchers, health administrators, policy wonks, and others. Not a single representative of psychiatric patients presented. But still, the picture painted of the system seemed as abysmal as that painted by patients in Virginia, as evidenced in the Committee’s April 2026 report.
All of these people working within the North Carolina involuntary commitment system described a litany of problems.
Law enforcement officers in North Carolina are often spending hours making calls and driving around trying to find a place to take a person they’ve detained.
Emergency department wait times are supposed to be no longer than four hours, but average 285 hours. Being stuck together in these uncomfortable, chaotic environments causes rising frustration and stress for both patients and staff as patients’ physical and mental conditions worsen—and this can sometimes boil over into danger and violence.
People brought in for a brief examination for possible commitment—even if they ultimately don’t get committed—are frequently immediately kicked out of their room in a nursing home, mental-health group home, or other site operated by local social services. Basically, many people who are detained instantly become homeless—and consequently then get held in these boiling-over emergency rooms “for weeks and months” while hoping a new place to live emerges.
Presenters said a significant percentage of detentions involve just a small number of the same people, repeatedly getting involuntarily committed and forcibly treated after being arrested for petty misdemeanors—and their situations never change for the better. This “revolving door” of ineffectiveness is exacerbated by the fact that the various branches of the involuntary commitment systems are meant to be working closely together, but in fact “do not talk to each other.”
The costs of this inept, failing system are staggering. According to Karen Burkes, North Carolina’s Deputy Secretary for Facilities and Licensure, a single typical facility for holding about 20 patients requires staffing with 17 registered nurses, 42 health care techs, and two psychiatrists. Basically, for every one person being detained, the system is paying three people full-time wages to do what often amounts to little more than babysitting that person.
All of this adds to an earlier report from Disability Rights North Carolina showing widespread misuses and abuses in the state’s involuntary commitment system, and findings that rates of involuntary commitment in the state have at least doubled in ten years.
And all of this is also dogged, once again, by a lack of evidence that any of it is actually helping anyone. Dr. Jeni Corn is Research Director of Social Sciences at the NC Collaboratory, which has been legislatively mandated to study these involuntary commitment processes and systems in North Carolina and make recommendations for improvements. Corn explained to the legislators that the main challenge for her team in doing their job is the complete “lack” of “relevant data” being collected across any state agencies, mental-health service providers, or judicial systems.
The fantasy of “the right treatment”
So, how does any of this make any scientific, policy or fiscal sense? One might think these testimonies would provoke North Carolina legislators to think outside the box; perhaps even to propose some radically new approaches.
But no, they do not propose stopping all involuntary commitment pending there being demonstrable evidence of its benefits.
Instead, throughout the report, the experts and committee members keep speaking about ensuring that people “receive the right care, at the right time, and in the right place” and “receive necessary treatment for their underlying issues.”

But what is this miracle psychiatric treatment approach that will assuredly improve everyone’s lives whether they like it or not? That is never questioned, discussed, or explored anywhere in the 42-page report.
The Committee simply recommends creating more spaces and places where people can be detained. Increasing the number and types of providers who can commit people. Expanding mobile crisis teams and allowing them to commit people, too. Using telehealth systems to make the commitment process faster. Hiring more staff to operate commitment facilities. Making more beds available, lowering wait times, and expanding outpatient commitment.
Throwing one bone to critics, the Committee did recommend collecting more and better data—but added that a primary goal of that effort would simply be to help expedite people getting more “timely” involuntary commitment.
So, what is this strange faith that makes politicians, even as they are being slapped repeatedly in the face with how inept, harmful, and expensive the involuntary commitment system is, keep believing that simply providing more funding and facilitating bigger expansions will suddenly make it work wonders? Why do people working in these systems themselves, well aware of how bad they are, not speak out more about the need for more radical changes? And why do so many think it’s acceptable for such abuses to be going on, instead of demanding an immediate cessation and truly substantive changes?
Might the answers to those questions also explain why involuntary commitment systems tend to be so bad?
“People brought in for a brief examination for possible commitment—even if they ultimately don’t get committed—are frequently immediately kicked out of their room in a nursing home, mental-health group home, or other site operated by local social services. Basically, many people who are detained instantly become homeless.” Wow, man. As homelessness is increasingly criminalized and facilities are built to incarcerate surplus humanity (that which does not generate profit for the Epstein class), not getting committed will more and more mean getting committed to someplace else at least as bad, I guess.
“Many reported that they were not able or not allowed to attend their own commitment hearings, and some said they didn’t even get hearings. Some were so heavily medicated against their will that they could not stay awake for their own hearings” - so gross. Kind of sums up the concept of mental patients' "rights" as the bitter joke that it is. Of course, "rights" are now being exposed as something that was only ever meant to serve the ruling class.